Benefits

1. Reduced inpatient stay
Robotic surgery extends the benefits of conventional laparoscopy (decreased length of stay, decreased blood loss, decreased pain, quicker return to activities, and improved cosmetic result through smaller incisions[1, 2]) to a much wider group of patients requiring more complex reconstructive procedures.
In United States they have compared the outcomes of robotic surgery compared to laparoscopic and open surgery nationwide, across common procedure types, there was a significant decrease in the length of stay and likelihood of mortality for the robotic surgery group when compared to the open and conventional laparoscopic surgery groups[3].
The limitations of traditional laparoscopy include; two-dimensional vision, poor dexterity due to the fulcrum effect, the transmission and amplification of the surgeon’s hand tremor. This prevents it from being used more widely amongst paediatric patients[4]. A robotic approach would allow the benefits of minimally invasive surgery to be extended to a much wider population of patients.
Many children with neuropathic bladder, posterior urethral valves and bladder exstrophy require bladder augmentations. Currently this is done via the open approach and the post-operative inpatient stay is usually between 7-10 days. Robotic surgery has been shown to reduce the inpatient stay to 6 days[5].
2. Improved recovery
In paediatric urology there is evidence that robot-assisted pyeloplasty may be superior to open and laparoscopic approach in terms of decreased length of stay, decreased narcotic use, and decreased operative times[6, 7]. In children undergoing bladder augmentation using a robotic approach epidurals were no longer required compared to those having an open approach, as patients were more comfortable and recovered more quickly[5]. Neheman et al compared the outcomes of robotic and laparoscopic pyeloplasty and found that there was significant shorter inpatient stay with robotic surgery (p<0.0001)[8].
3. Fewer complications
Increasing numbers of paediatric publications have compared the outcomes of robotic procedures to open surgery. These include appendicovesicostomy[9], ureteric reimplantation [10], bladder neck reconstruction [11], placement of bladder neck sling[12], excision of bladder diverticulae [13], bladder augmentation[14], resection of Wilm’s tumour[15], reconstruction of vaginal atresia[16], repair of congenital diaphragmatic anomalies[17], thoracic surgery[18] and Hirschsprungs pull-through surgery[19]. All of these studies show that a robotic approach can be safely employed in children to achieve the same outcomes as open surgery with shorter inpatient stays and quicker recovery.
A significant complication following laparotomy is adhesive bowel obstruction occurring in up to 20% of patients. A robotic approach results in reduced peritoneal attachments following ileocystoplasty compared to an open approach approach[20]. Robotic ileocystoplasty has now been performed in a paediatric population safely and with at least comparable outcomes to the open approach[5, 14].
Heminephrectomy using segmental arterial mapping performed robotically reduces the chance of injury to the normally functioning part of the duplex kidney[21]. Robotic surgery has become a standard approach for heminephrectomy in adult urology and is now becoming accepted as best practice amongst paediatric patients.
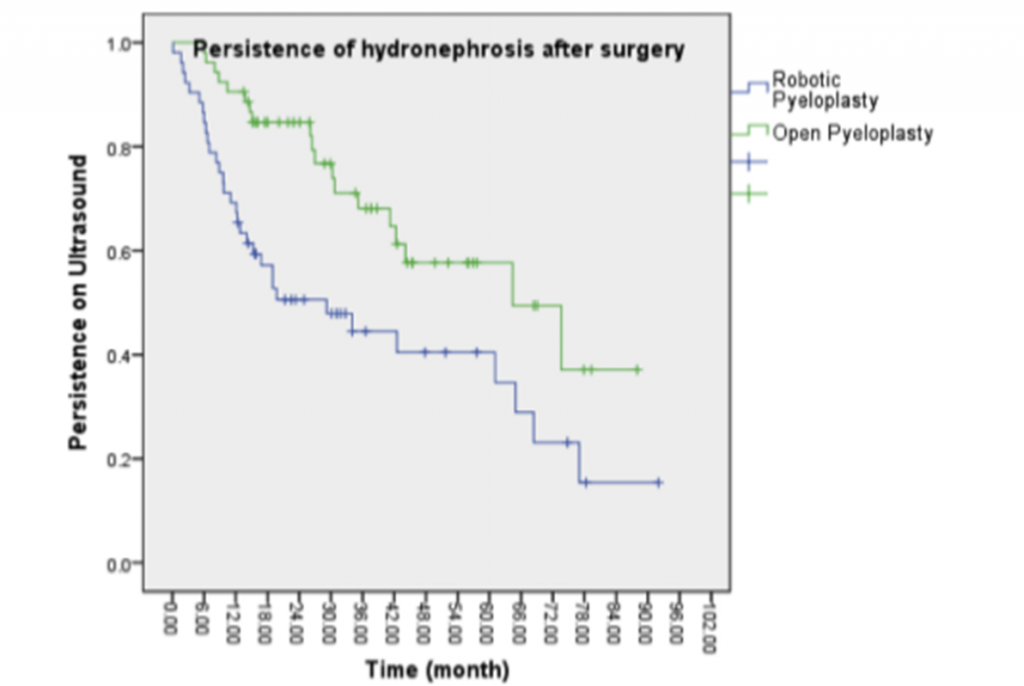
Following pyeloplasty the success of surgery is measured by resolution of dilatation (hydronephrosis). In a review of 212 pyeloplasty operations a comparison of open versus robotic pyeloplasty found that complete resolution of hydronephrosis was higher in the robotic group compared to the open group (62% vs. 45%) [22].
A shorter time to improvement was seen with robotic pyeloplasty (12.3 months vs. 29.9 months) compared to conventional open pyeloplasty. Silay et al found that patients undergoing robotic pyeloplasty had a shorter inpatient stay of 2.1 days compared to 4.6 days in those undergoing laparoscopic pyeloplasty (P=0.001) , they also had a reduction in postoperative complications of 3.2% compared to 7.7% (P=0.02)[23].
Fig 4: Kaplain Meier chart describing persistence of hydronephrosis after robotic surgery (blue line) and open surgery (green line)
4. Enhanced learning curve for surgeons in training
Robotics enhances the early learning curve for novices when performing complet tasks such as knot tying when compared to standard laparoscopic tools. For experts, robotics is most useful for improving economy of motion for the highly complex procedures in limited workspaces[24], such as that seen in children.
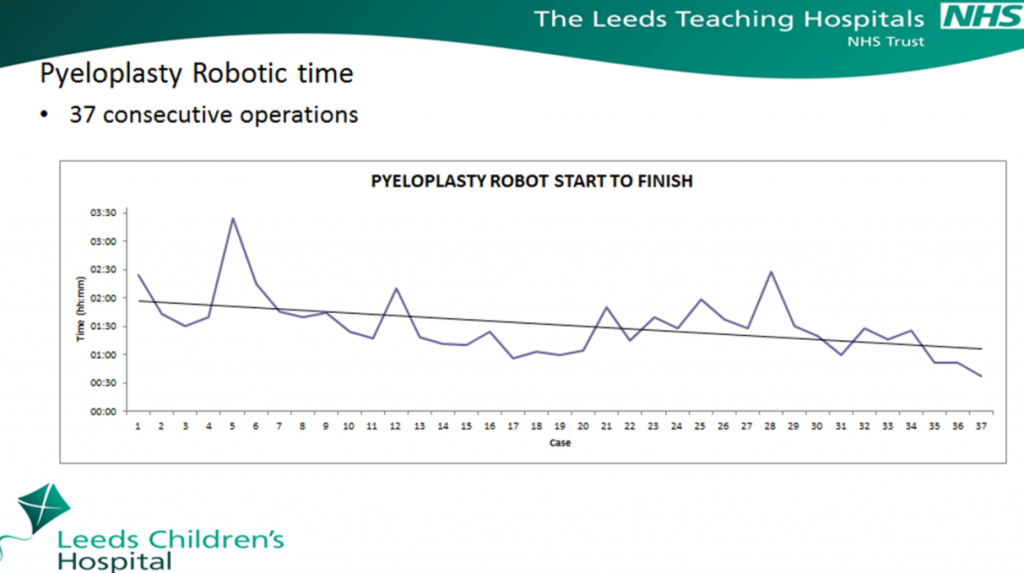
Robotic surgery also improves technical performance and enhances prefrontal activation during suturing compared to standard laparoscopic tools[25]. Tasian 2013 demonstrated that the operative times were similar to an experienced robotic surgeon after 37 cases[26] (Fig 5). The Leeds experience demonstrated similar findings with operating times approaching open surgery after 30 cases (Fig 6).
Fig 5: Graph detailing operative times in robotic pyeloplasty procedures performed by fellows compared to an experienced robotic surgeon. After 37 robotic pyeloplasties this reached the 58 minutes representing the median operative time of an experienced robotic surgeon[26]
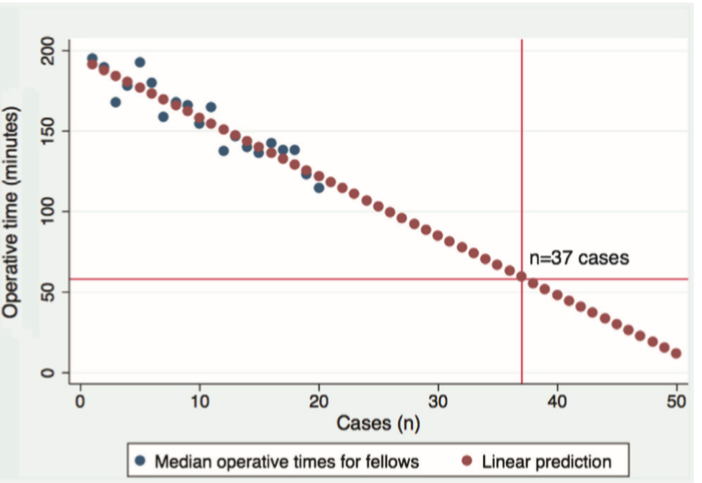
Fig 6: Pyeloplasty Procedure Times. As surgeons and theatre teams are trained the procedure times gradually reduce as can be seen by the Leeds robotic experience: